![[TTL]](/clients/sonoskills/themes/uploads/crop_1574086706Schermafbeelding20191118om15.12.35.png)
Calcific tendinopathy is a common disorder related to the deposition of calcium hydroxyapatite crystals within the tendons which has three stages: precalcific, calcific, and repair stage. The calcific phase can be further subdivided into formative, resting, and resorptive phase (1, 2, 3, 4) . Other names have been given to this pathology, such as calcific tendinosis, calcifying tendinitis, tendinous calcifications, calcium hydroxyapatite crystal deposition disease, etc. (4) .
Why?
The pathogenesis is not completely understood, but it seems to be related to areas of hypoxia in tendons that lead to fibrocartilaginous metaplasia and cellular necrosis, followed by the formation of a calcium deposit, typically in an intact tendon (1, 2) . Hormonal disorders are also mentioned in the literature (3, 4) .
Where?
It could occur in any tendon, although some tendons are more predisposed to it. In the shoulder the supraspinatus is the most involved tendon (80 %), followed by the infraspinatus (15 %) and subscapularis (5 %) (4) .
Who?
This condition has been reported in 2.5–7.5% of healthy shoulders in adults, occurring in women in about 70% of cases (2) .
When?
Especially during the fourth and fifth decades of life. It does not seem to be related to physical activity (2) .
Pain
In the initial stages, the patient is usually asymptomatic, although large calcific deposits may cause mechanical symptoms (3) . Pain can be caused by several factors (1) such as:
a) calcium causing chemical irritation of tissues;
b) tissue edema causing pressure;
c) bursal thickening due to irritation causing impingement;
d) pain caused by chronic stiffening of glenohumeral joint.
Although considered a self-healing condition, it can cause acute/chronic pain and functional disability depending on the stage of the disease (2) . Most pain will be felt in the resorptive phase of the calcific stage in which the patient may feel local excruciating pain and severe limitation of movement. Hyperesthesia of the surrounding skin and redness are noted when migration involves superficial structures. A low-grade fever may be present. Clinical symptoms are characteristically the worst in the first days and gradually disappear in 2 to 3 weeks (1, 3) .
1 - Precalcific stage
In this stage a fibrocartilaginous transformation, probably related to decreased oxygen tension, occurs within tendon fibers and is usually asymptomatic (2, 3) .
2a - Calcific stage: formative phase
Calcifications are formed, usually poorly symptomatic. Subacute low-grade pain increasing at night can be felt (2) .
2b - Calcific stage: resting phase
Homogeneous and well-defined calcifications, contained within the tendon, can be found (3) .
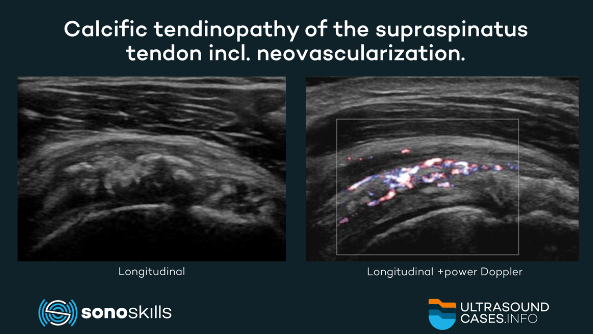
2c - Calcific stage: resorptive phase
A cellular reaction around the calcific deposits can be found. Increased vascularity of the tendon occurs, and the deposits grow in size and become poorly defined (2) . The tendon develops increased vascularization and calcium deposits are usually removed by phagocytes. Calcifications may migrate into the adjacent structures which causes local excruciating pain and severe limitation of movement (3, 4) .
3 – Repair stage
Self-healing and repair of the tendon fibers occurs due to granulation tissue with fibroblasts who start to remodel the tendon (3) . This lasts for several years and may be associated with pain and restricted function (2) . As the process proceeds, fibroblasts and collagen may align along the long axis of the tendon (3) .
Migration
In the resorptive phase of the calcific stage it is common for hydroxyapatite deposits in tendons to migrate to adjacent tissues, such as bursae, and less frequently to bones. However, migration of hydroxyapatite crystals along the tendon toward the myotendinous junction has been described in only few cases (2) . Intramuscular migration of calcium deposits is rare (4) . The exact cause of the migration is unknown (3) . It is hypothesized that migration may be related to intrasubstance delaminating-type tendon tears that provide a pathway for the calcifications (4) .
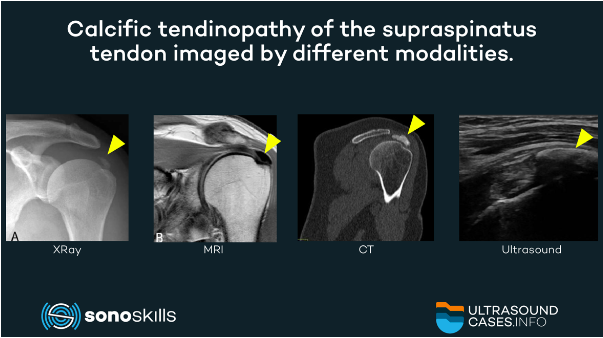
XRay, MRI, and CT
- XRay: most commonly used. XRay evaluation of shoulder is done by 2 views (3) . Its drawbacks are ionizing radiation and high cost (4) .
- MRI: has well-known limitations in assessing intra-tendinous calcifications. It also is expensive (4) . Nevertheless, it is the only technique to assess bone edema in intraosseous calcium migration (3). Nevertheless, it plays a role in the identification and localization of calcific deposits within the cuff, surrounding edema, associated pathologies of rotator cuff as complete or partial tears, presence of sub acromial bursitis (1) .
- CT: is superior in comparison to musculoskeletal ultrasound (MSKUS) in showing deep-tendon calcifications or the deeper surface of a calcification. It is also superior to radiographs in cases of superposition of adjacent bones to spatially localize the calcification (1) .
MSKUS has been shown to be an excellent imaging modality for the evaluation of calcific tendinopathy: it can show calcifications inside most of the appendicular tendons (3) .
MSKUS using longitudinal and transverse views determines size, localization, echogenicity of the deposits and associated rotator cuff tear (1) . Calcific deposits, at least the superficial surface, most commonly appear hyperechoic. Color Doppler is more descriptive about the vascularity (1) . Color Doppler imaging is mostly associated and correlates well with patients’ symptoms (3).
Calcific tendinopathy should be differentiated from other types of soft tissue calcifications such as enthesopathy, avulsion fractures at tendon attachments, rheumatology diseases and aggressive calcified lesions (3) . Dynamic scanning during shoulder movements may also show an incomplete gliding of the involved tendon and muscular belly due to the calcific deposits (4) . One author recommends, during an MSKUS-examination in particular in calcific tendinopathy, to check systematically not only the tendons, but also the muscle bellies of the rotator cuff (4) .
MSKUS can be used for diagnostic, prognostic, interventional purposes and evaluative purposes. To scan patients non-invasively, real-time, functional and with low costs. An MSKUS guided intervention could be a local anesthetic/steroid injection in the resorptive phase, when indicated (3) .
Classification
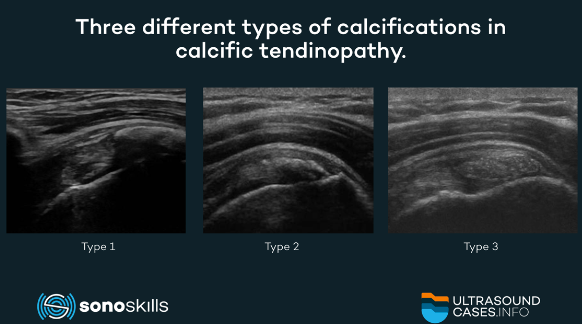
Three types (1, 3) have been described, based on the percentage of calcium in the deposits:
- Type 1: dense calcifications with a well-defined border. Calcifications are rich in calcium and correspond to the formative and resting phases; MSKUS shows them as hyperechoic structures with well-defined acoustic shadowing.
- Type 2: dense with Indefinite borders. Calcifications are hyperechoic but show a faint acoustic shadow.
- Type 3: transparent with indistinct border. No acoustic shadow is seen in Type 3 calcifications.
Types 2 and 3 generally correspond to the resorptive phase in which the calcium deposit appears poorly defined. Type 3 calcifications may be isoechoic to tendons, an appearance that may be misleading for novice sonographers and lead to under detection of the calcifications (3, 4) . The calcium deposit in type 2 and 3 may be semiliquid (4) .
References:
- Umamahesvarana B, Sambandamb SN, Mounasamyc V, Gokulakrishnana PP, Ashraf M. Calcifying Tendinitis of Shoulder: A Concise Review. Journal of Orthopaedics 15 (2018) 776–782. DOI: 10.1016/j.jor.2018.05.040. Free full text article: http://bit.ly/2qdLewD
- Cocco G, Ricci V, Boccatonda A, Iannetti G, Schiavone C. Migration of calcium deposit over the biceps brachii muscle, a rare complication of calcifc tendinopathy: Ultrasound image and treatment. Journal of Ultrasound 21 (2018) 351-354. DOI:10.1007/s40477-018-0336-z. Pubmed: http://bit.ly/356u8zT
- Bianchi S, Becciolini M. Ultrasound Appearance of the Migration of Tendon Calcifications. Journal of Ultrasound in Medicine 38 (2019) 2493-2506.DOI:10.1002/jum.14933. Pubmed: http://bit.ly/2Ivdh0y
- Becciolini M, Bonacchi G, Galletti S. Intramuscular migration of calcific tendinopathy in the rotator cuff: ultrasound appearance and a review of the literature. Journal of Ultrasound. 19 (2016) 175-81. DOI: 10.1007/s40477-016-0202-9. Free full text article: http://bit.ly/2XhMdIj